ICSI is done as a part of IVF. Since ICSI is done in the lab, your IVF treatment won’t seem much different than an IVF treatment without ICSI.
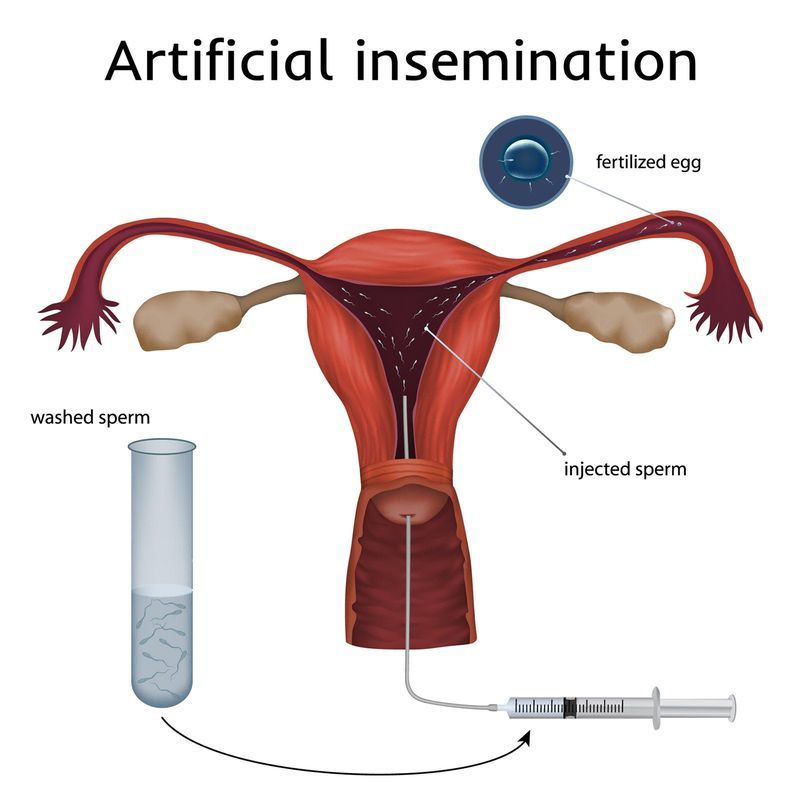
As with regular IVF, you’ll take ovarian stimulating drugs, while your doctor will monitor your progress with blood tests and ultrasounds. Once you’ve grown enough good-sized follicles, you’ll have the egg retrieval, where eggs are removed from your ovaries with a specialized, ultrasound-guided needle.
Your partner will provide his sperm sample that same day (unless you’re using a sperm donor, or previously frozen sperm.)
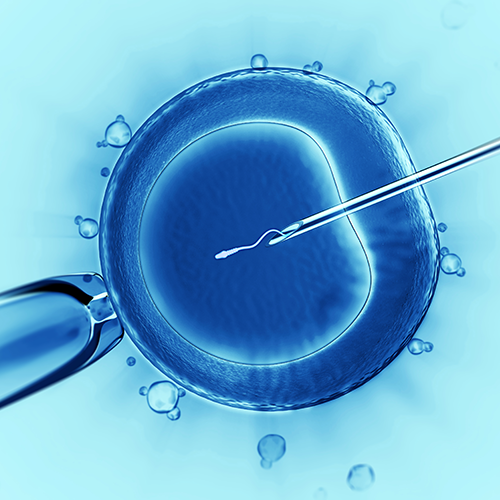
Once the eggs are retrieved, an embryologist will place the eggs in a special culture, and using a microscope and tiny needle, a single sperm will be injected into an egg. This will be done for each egg retrieved.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}